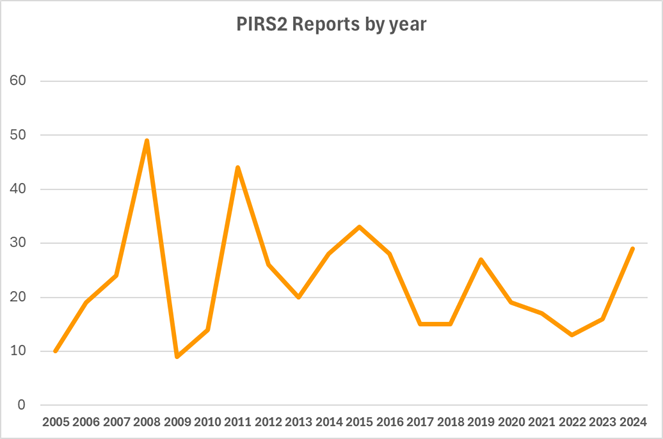
Pleasingly there has been an 80% increase in reports to PIRS 2 for 2024 over 2023 following a decreasing trend in numbers prior to that. At the recent ASCVP Annual Scientific Meeting following a presentation on PIRS2 there was discussion on barriers to reporting. One comment was that editorial commentary could be one such barrier.
The purpose of the editorial commentary – reserved for some reports – is to provide helpful information and promote discussion. The PIRS2 Report submission form Q22 asks for “ Permission to publish edited description in ANZCP Gazette &/or website”. We will add – “and to circulate to the PIRS2 email group”
It is very appropriate to submit a report and answer NO to permission to publish. In a case the deidentified data will simply go into the data base and the relevant categories and human factors used in analyses. Descriptive details will remain embargoed. This may give comfort to those hesitant to report.
Timothy W. Willcox, CCP;* Robert A. Baker, PhD, CCP^
*Green Lane Cardiothoracic Unit, Auckland City Hospital, Auckland, New Zealand; and Department of Anaesthesiology, School of Medicine, University of Auckland, Auckland, New Zealand; and ^Cardiac and Thoracic Surgery Unit, Flinders Medical Centre, Adelaide, South Australia; College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia.